
In January 2015, Aubrey Reinhardt came to an important conclusion: It was time to get on birth control.
The 20-year-old Texas Tech University senior was in a serious relationship, and after a prudent discussion with her partner, she’d made up her mind. Analytical by nature, Reinhardt sought information on her options and narrowed down the list of contraceptives she wanted to know more about. Ultimately, that might have been the easiest part of the process.
Through friends and family, she knew that Planned Parenthood was a trusted source for reproductive health care, but in the Panhandle city of Lubbock, that would not be an option. The university town’s two Planned Parenthood clinics had closed down in 2014, the result of a series of ill-fated political decisions made by state lawmakers hellbent on fully defunding the 100-year-old provider.
Reinhardt asked around and was told that the university’s medical center was now the go-to for birth control. On a cloudless, cold winter day, she and a friend headed to campus to see the doctor. It did not go well. After assessing Reinhardt’s medical history, the doctor said she believed Reinhardt had a blood-clotting problem and was “too unhealthy” to be on birth control. While it is true that Reinhardt had a minor health scare the year before, any clotting problems had been ruled out before she underwent surgery to address the issue. Reinhardt was stunned. “I thought, Where the heck is this coming from?” she recalled recently. “This is bizarre to me, but I’m thinking, OK, she’s a medical professional … and I’m a kid and I’m trusting her.”
The doctor said she would consider prescribing contraceptives, but only if Reinhardt would get her primary care doctor and her surgeon to fill out packets of paperwork. She would also have to visit a hormone specialist and request additional documentation. “I was as baffled as you are right now,” she said. When the doctor left the room, Reinhardt and her friend tried to figure out what had just happened. “I’m getting a little bit emotional because I’m like, this is a bombshell that’s just been dropped on my life, like I must be very ill and I just don’t even know it.”
When the doctor returned and saw Reinhardt crying, she was scornful. “’Why are you so upset, why are you crying? Are you really in that big a hurry to become sexually active?’” Reinhardt recalled her saying. “And that was the moment that … everything clicked with me: This isn’t an issue with my health, this is an issue of a doctor who doesn’t agree with what I’m wanting.”
Reinhardt tried to contact a reproductive health clinic that had promised it would pick up the slack after Planned Parenthood left town, but it had already folded its operations. She tried another provider but was told it would take four months to get an appointment. Frustrated and angry, Reinhardt called Planned Parenthood — maybe there was a clinic somewhere nearby and she just wasn’t aware of it. No, she was told, there wasn’t a clinic anywhere in the Panhandle, an area more than twice the size of Massachusetts. The two closest clinics still open were four hours southwest, in El Paso, and four hours east, in Fort Worth.
Reinhardt ended up getting an implanted, long-acting contraceptive in Fort Worth — without needing additional paperwork from her primary care doctor, her surgeon, or a hormone specialist. She understands that for all she had to go through to get the birth control she wanted, she was still fortunate: She had the resources and support to make it happen. But she worries about those who don’t have the same advantages — women whose ranks have grown since 82 reproductive health clinics across the state closed in response to legislative actions, a third of which were Planned Parenthood clinics. “People are going without health care,” she said. “Even though I’m sitting here upset, I know there are people who are also upset and in more dire situations.”
Reinhardt’s assessment is on target: 16 percent of Texans live below the federal poverty line, and at 24 percent, the state has the highest percentage of uninsured women of reproductive age.
But instead of finding realistic ways of expanding access to accommodate this need, state officials have focused their efforts on defunding their ideological foe, Planned Parenthood. This has taken several forms, the most obvious of which is the passage of many onerous restrictions on abortion care. But perhaps even more destructive is the decision to bar Planned Parenthood from participating in any state-funded health care programs, regardless of the fact that none of those funds pay for abortions. In that arena, Texas has been entirely successful — even if it has also drastically reduced the ability of low-income women to access subsidized care.
To date, Medicaid funding is the only remaining pot that the state has been powerless to withhold from Planned Parenthood. That is primarily because the federal fee-for-service program contains a provision ensuring that recipients are able to seek care from a provider of their choice. The provision mandates that recipients may seek services from any provider qualified and willing to furnish them.
In an April 2016 advisory to state Medicaid officials, Vikki Wachino, then-director of the Centers for Medicare and Medicaid Services, housed under the U.S. Department of Health and Human Services, wrote that states “may not” act on a “desire to target a provider or set of providers for reasons unrelated to their fitness to perform covered services.” In other words, states can’t block Planned Parenthood clinics from providing birth control and pelvic exams just because they don’t like that some clinics also offer abortion services.
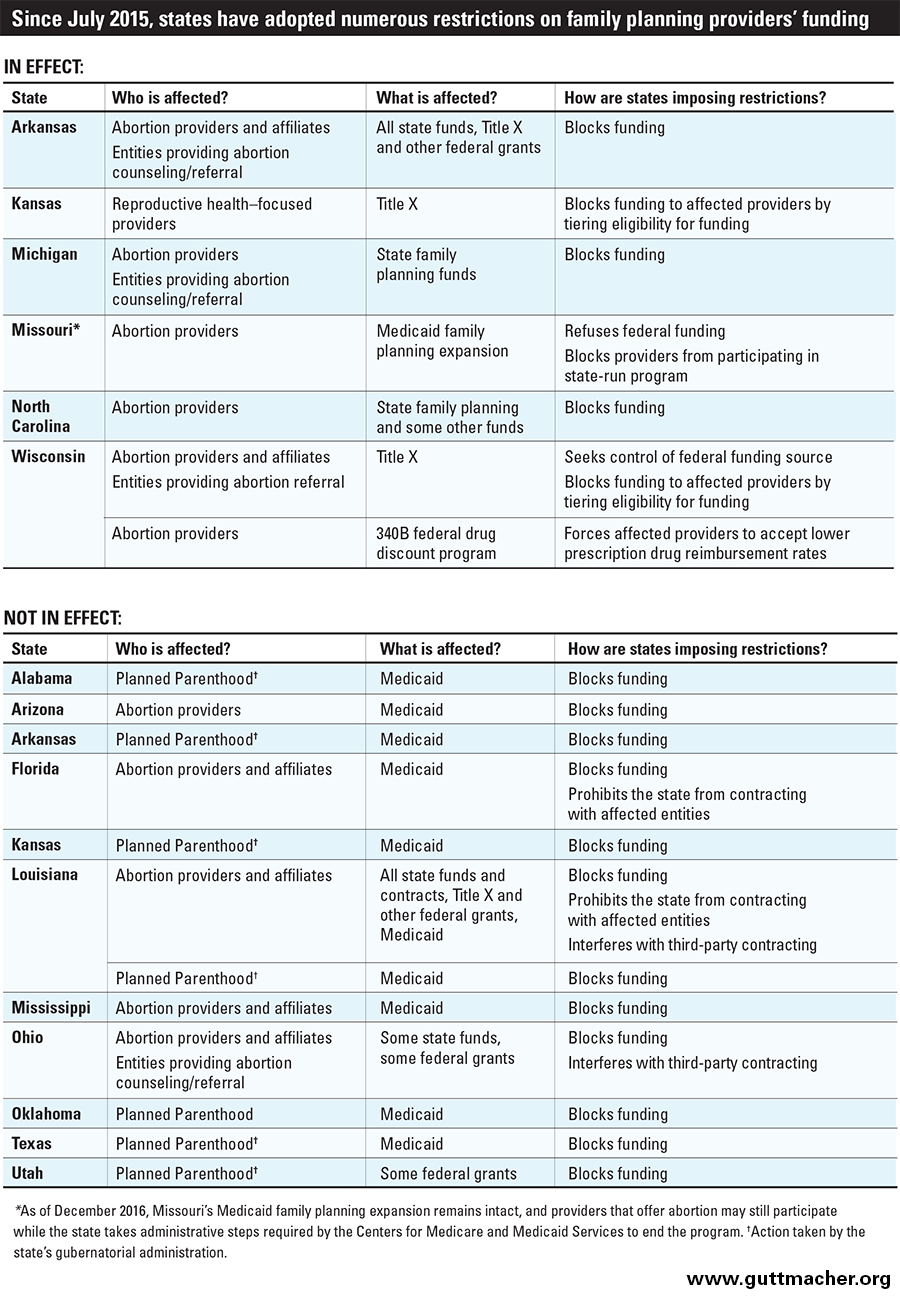
The “clarifying” letter was timely. Over the last few years, a number of states have tried to ban Planned Parenthood from Medicaid by claiming it’s not qualified to provide care based on widely discredited videos that purport to show Planned Parenthood officials selling fetal tissue. A federal judge blocked Texas’s attempt to do this earlier this year. Only one state hasn’t yet been blocked in this effort. On August 16, a panel of federal judges cleared the way for Arkansas to withhold funds from the provider. Whether that ruling will stand remains to be seen.
Texas, however, remains unbowed. In its application for a so-called Medicaid waiver program, the state is seeking to circumvent previous court rulings by asking the federal government to waive the freedom of choice provision altogether. If the government grants the request, allowing the state to deny patients the right to choose where they receive care, Texas will have successfully drawn a roadmap for other ideologically driven states to follow in its footsteps, withholding millions in federal funds from the reproductive care giant and reducing access to health care for potentially millions of women.
Through a Medicaid waiver program, a state can receive permission to opt out of certain federal rules in order to try a new health care delivery model. Typically, this involves waiving some of the financial eligibility requirements in order to expand the patient pool.
Ten years ago, Texas did exactly this when it asked to expand access to reproductive health care for women not poor enough to qualify for Medicaid unless they were pregnant. Under the program, for every $1 Texas put in, the feds would kick in $9.
It was a good financial deal for the state and intended not only to expand access to birth control and related care, but also to decrease the number of unintended pregnancies paid for by Medicaid — a significant issue in Texas, where the program pays for more than half of all births.
Known as the Women’s Health Program, the pilot got off the ground in 2007, and with concerted effort, it grew quickly. In 2008 alone, the program reduced the number of unintended pregnancies that Medicaid would have paid for by more than 10,000, saving more than $92 million in costs to both the state and federal governments. By the end of 2011, the program’s enrollment surged to nearly 130,000, with 90 percent of those women accessing the covered services. By all measures, the program was working.
But lawmakers were unhappy. Planned Parenthood was serving more than 40 percent of the program’s clients, making it the single largest provider of WHP services. So they crafted a new rule that would ban any entity “affiliated” with an abortion provider from participating in the program.
Blocking Planned Parenthood would violate Medicaid’s provider of choice provision, the federal government told the state in late 2011. Unless Texas lifted the new affiliate rule, its application to renew the program would be denied. The state refused, foregoing federal funding and claiming it could run the women’s health program just fine on its own.
That did not turn out to be true. From 2011 through 2016, the program was twice rebranded and enrollment dropped 24 percent. Over the same period, there was a 39 percent drop in the number of women in the program who were actually receiving services. Equally troubling, the number of women able to access birth control dropped 41 percent, according to a new study from the Center for Public Policy Priorities in Austin.
Research from the Texas Policy Evaluation Project, housed at the University of Texas’s Population Research Center, found that in the wake of the policy changes that ousted Planned Parenthood (and other smaller clinics), the number of women receiving long-acting reversible contraceptives, like the one Reinhardt received, decreased by 35 percent. And the number of women receiving injectable contraceptives declined by 31 percent, while the number of Medicaid-paid pregnancies among this group subsequently rose by 27 percent.
These numbers have not fazed Texas lawmakers, who continue to insist that they know how to run a successful women’s health program that excludes the single highest-volume supplier of care — going so far as to force a director at the agency overseeing the program to retire for having participated in research that proved the exclusion actually restricted access to care.
The state points to a dramatic increase in enrollment and the number of participating providers over the last year — up to 202,584 women enrolled in June and 5,342 providers signed up to participate — as some proof of the program’s success. But there are major caveats. First, enrollment rose because the state is now automatically extending coverage for mothers who’ve just had a Medicaid-paid birth. That’s a great thing, says Stacey Pogue, who ran the WHP in its first years and is the author of the CPPP’s latest report, but she is concerned that without clear direction from the state, those women might not be aware of the program or the fact that they’re covered by it. And even if they are, “that doesn’t mean they’ll ever get services,” she said.
That is because although the raw number of providers has increased dramatically — to include a number of individual doctors — many of them don’t actually see clients. Analysis of state data Pogue and colleagues did several years ago revealed that more than 50 percent of program providers saw “zero or one woman” annually, she said.
And there’s nothing to suggest that has changed. The latest incarnation of the program — now known as Healthy Texas Women — started in the summer of 2016. It is unclear how many clients have been served to date. An April report from the Health and Human Services Commission revealed that just over 60,000 women had received services through February; a report from May omits data about the current fiscal year.
And news about at least one of the organizations awarded a hefty contract by the state has raised eyebrows. The Heidi Group, granted more than $1.5 million under Healthy Texas Women, has no experience in providing women’s health care. Carol Everett, its founder and CEO, is an anti-abortion activist who has run a network of crisis pregnancy centers that exist primarily to encourage women to carry unwanted pregnancies to term.
Everett’s group said it could serve slightly more than 50,000 women with the state grant — a number that is shocking to Pogue and others. “That is an astounding number,” Pogue said. “That is more than Planned Parenthood served when it had 51 clinics in the program.” The Heidi Group has fewer than two dozen clinics and doctor’s offices signed on to provide care. At least one of the providers the group has contracted to serve the program’s clients is a crisis pregnancy center, Wise Choices, which does not provide birth control — let alone any other medical services.
Despite its mediocre track record at ensuring low-income women have access to birth control and other preventive health care, Texas is applying with the feds to transform Healthy Texas Women into a Medicaid waiver program, a move that would unleash millions in federal funding. But instead of just asking for a waiver to increase eligibility, this time the state is also asking that the government waive the program’s provider of choice provision.
There is reason to think that Texas’s bid to do away with freedom of choice could be successful — not least of which is that it appears the feds approached the state to ask that it reapply for the funding. Carrie Williams, press officer for the Texas Health and Human Services Commission, acknowledged as much to the Houston Chronicle. She wouldn’t say who was nudging the state, only that “the sentiment is that the federal government may be open to new ideas.”
Under President Donald Trump, the Department of Health and Human Services has taken a decidedly hostile attitude toward women’s health. Secretary Tom Price infamously asserted that women don’t need help to access birth control. To run the nation’s family planning program, the president tapped an anti-abortion crusader, Teresa Manning, who doesn’t believe that birth control works.
His pick to run the Centers for Medicare and Medicaid Services, Seema Verma — an ally of Vice President Mike Pence — is perhaps best known for using a Medicaid waiver to create a program in Indiana that actually restricted access to care and made some enrollees pay premiums.
In March, Verma told a group of female health care professionals that “as a mother and as a woman, the most important thing about my health care is being able to pick out the doctor that I feel comfortable with.” Still, women’s health advocates are concerned that she may not feel the same way about low-income women who need Medicaid in order to access care.
“The Texas waiver request is a new attempt to circumvent federal protections for women’s health,” Clare Coleman, president and CEO of the National Family Planning and Reproductive Health Association, said in a statement. “A CMS approval of Texas’s waiver would perpetuate a failed experiment. Women should have the ability to choose the health provider that they know and trust … regardless of income level.”
Technically, the freedom of choice provision can be waived, but “you can only waive that provision if doing so furthers the goal of the Medicaid program,” says Pogue. And it has never before been waived in connection with a family planning program. “A state has never come and said, we have a more efficient network if we just go with these” few, limited providers, she said. Certainly, Texas has demonstrated that “there is no benefit” to waiving the choice provision. “You cannot further the goals of Medicaid by excluding your most efficient provider.”
Pogue and others worry that if the federal government breaks precedent and waives freedom of choice for reproductive health, it would encourage other states to seek to do the same. Since 2015, at least 10 states have tried to block Planned Parenthood from receiving any Medicaid funds.
{kind=link}
Texas “has spent years crippling a once-successful program supporting family planning and related services for low-income residents,” Kinsey Hasstedt and Adam Sonfield with the Guttmacher Institute wrote in July for Health Affairs Blog. “Now, the state is asking the likeminded Trump administration to provide an infusion of federal funding to support its diminished program. In the process, Texas and the Trump administration could set dangerous new precedents that could undermine family planning care in Medicaid programs nationwide.”
Indeed, Pogue notes that if the state is successful, it won’t be Texans who are hurt: The damage to the state’s health care safety net has already been done. Rather, the victims would be women in other states where access to care could be devastated, as it has in Texas. “I think the real point is, when Texas told itself a story … of ‘we can exclude a provider for whatever reason and our program will be fine, and women’s access will be fine because there are other providers to pick up the slack,’ it turns out that is not true,” she said.
There are two paths here and they are “mutually exclusive,” she notes. You can kick out a trusted, high-volume provider like Planned Parenthood and decrease access to services. Or, you can increase access and have a thriving program. “But you can’t do both.”
“That’s what Texas said they could do,” she said, “and that’s certainly not what the Texas experience shows.”
For Reinhardt, the experience of trying to access birth control in the wake of the closures of Planned Parenthood clinics in Lubbock stayed with her.
She’s in law school now, in North Texas, where she founded a chapter of the reproductive justice group If/When/How, and has become a passionate advocate for Planned Parenthood and the expansion of reproductive care access.
She worries the federal government will approve Texas’s waiver but still has hope it will see such a decision as a disaster in the making. “Plenty of states look to Texas for guidance on these kinds of policies, and it’s alarming,” she said. “This may have happened to me two years ago, but not only am I feeling the repercussions of this, but other people are too — and they’re still experiencing these issues every single day throughout Texas.”
The post Texas Seeks Trump’s Help to Defund Planned Parenthood. If It’s Successful, Other States Could Follow. appeared first on The Intercept.